Are you sure you want to exit?
The information you’ve provided will not be saved.
CTCL Staging Tool
This tool is intended for educational purposes only and to be used by qualified healthcare professionals (HCPs). HCPs remain responsible for diagnosing and treating patients in accordance with their clinical judgment.
Unlike other lymphomas, staging Mycosis Fungoides (MF)/Sézary Syndrome (SS) follows the TNMB system, which evaluates the extent of the disease across 4 compartments: skin (T), lymph nodes (N), visceral/metastasis (M), and blood (B).1 Each compartment is assessed separately to determine the severity and distribution of the disease for staging.
This tool will guide you on what to look for when staging patients with MF or SS.
The staging tool is based on consensus guidelines (ISCL, EORTC, USCLC, and NCCN). This tool was developed by Kyowa Kirin in consultation with CTCL experts.
 Blood (B)
Lymph nodes (N)
Visceral/
Blood (B)
Lymph nodes (N)
Visceral/metastasis (M)
TNMB stage
Expected time to complete: 5 minutes
- Skin (T) classification: up to 5 questions
- Lymph node (N) classification: up to 6 questions
- Visceral/metastasis (M) classification: up to 5 questions
- Blood (B) classification: up to 4 questions
MF/SS Diagnosis
Has the patient received a diagnosis consistent with Mycosis Fungoides (MF) or Sézary Syndrome (SS)?
-
Diagnosis of CTCL is complex, and can be challenging due in part to the
rarity
and heterogeneity of the disease1
- MF and SS may mimic common inflammatory skin conditions (eg, atopic dermatitis, psoriasis)
-
Keep in mind that there is no single test for diagnosing MF or SS;
accurate
diagnosis is based on correlation of clinical, histopathologic, and immunohistochemical
findings, as
well as T-cell receptor rearrangements2
- Confirmation of MF or SS requires correlation of clinical signs and symptoms with dermatopathological findings
- Pathologic evaluation of skin biopsy is a critical step in diagnosing MF and SS
- If skin biopsy results are inconclusive and/or discordant with clinical presentation, repeat biopsies over time may be helpful for definitive diagnosis
- In some cases, T-cell receptor (TCR) gene rearrangement studies may be helpful for diagnosis
- Consensus guidelines recommend consulting a specialist with expertise in CTCL if the patient has, or is suspected to have, MF or SS2
- For more information on the diagnosis of MF and SS, consult NCCN clinical practice guidelines
A diagnosis consistent with MF or SS is
needed for accurate staging3
Continue without complete compartmental information?
Skin (T) Classification
Question 1
Does the patient have widespread, diffuse erythema?
- Widespread erythema may be indicative of advanced stages (eg, erythrodermic Mycosis Fungoides [MF] or Sézary Syndrome [SS])1,2
Examples of erythema


Images are intended to be an example. Actual presentation may vary depending on individual patient factors.
Images provided courtesy of Oleg Akilov, MD, PhD.
- Widespread erythema may be suggestive of blood involvement1,2
- International ISCLC/USCLC/EORTC consensus guidelines recommend flow cytometry to assess blood involvement in MF and SS1 (more detailed information on flow cytometry is provided in the next section)
Skin (T) Classification
Question 2
Does the erythema affect ≥80% of the patient’s body surface area (BSA)?
- Erythroderma, defined as reddened skin covering ≥80% of BSA is suggestive of erythrodermic Mycosis Fungoides (MF) or Sézary Syndrome (SS)1,2
-
- Erythroderma is characteristic of SS, but may also be present in late-stage MF5
- International ISCLC/USCLC/EORTC consensus guidelines recommend blood evaluation (ie, flow cytometry) in addition to skin biopsy for accurate diagnosis and staging of MF and SS3 (more detailed information on flow cytometry is provided in the next section)
- Erythroderma is classified as T4 regardless of the presence of other types of skin lesions1
- In some cases, patients may have tumors, patches, or plaques in addition to erythrodermic skin3
Skin (T) Classification
Question 3
Are there tumors ≥1 cm in diameter present on the patient’s skin?
- Patients may have ulcerated or exophytic tumors, appearing as dome-shaped raised growths, which can be ulcerated and painful1
-
- Tumors are indicative of more advanced disease1,2
- NCCN consensus guidelines recommend consultation with a dermatopathologist or specialist with expertise in CTCL for optimal management of MF or SS5,6
Examples of tumors in a patient with MF


Images are intended to be an example. Actual presentation may vary depending on individual patient factors.
Images provided courtesy of Oleg Akilov, MD, PhD.
- Tumors are classified as T3 regardless of number of tumors or the presence of other types of lesions (patches or plaques)1
Skin (T) Classification
Question 4
Are there patch or plaque lesions present on the patient’s skin?
- Skin lesions in MF often include patches or plaques, which can vary in size, thickness, color, and location4
-
- Patches are the most common initial skin lesions, and typically appear as flat, scaly discolorations1
- Plaques often appear as raised bumps or thick firm lesions that may have a scaly texture7
Examples of MF patch lesions



Examples of mixed MF patches and plaques

Examples of MF plaque lesions



Images are intended to be an example. Actual presentation may vary depending on individual patient factors.
Images provided courtesy of Oleg Akilov, MD, PhD.
- A mixture of patches and plaques may be present on the skin3
Skin (T) Classification
Question 5
Do the patches/plaques cover ≥10% of the body surface area (BSA)?
- NCCN and ISCL/USCLC/EORTC consensus guidelines recommend a complete skin examination to assess the percentage of affected BSA for staging5
-
- BSA can be estimated by using the palm plus all 5 fingers, which equals roughly 1% of BSA1
- For consistency, estimation of BSA should be performed the same way every time1
Regional areas of the body for assessment of total BSA1
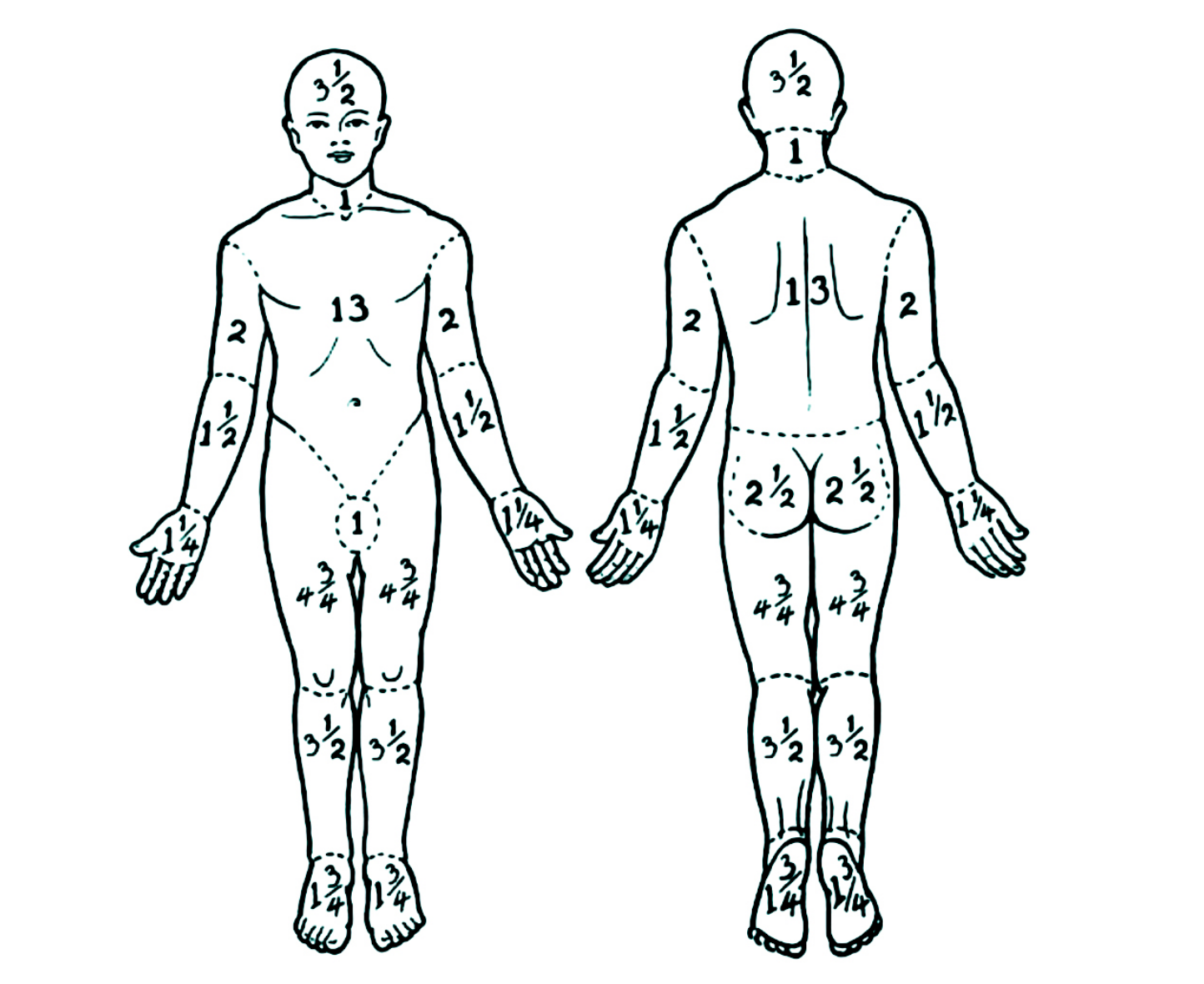
Adapted from Olsen et al (2007).2
- T classification is determined by the percentage of skin involvement as well as type of lesion1
- In general, if ≤10% BSA is affected by patches and/or plaques, skin is classified as T1, while ≥10% BSA is classified as T21
Skin (T) Classification Result
Based on NCCN and ISCL/USCLC/ EORTC consensus guidelines and the information you provided, this patient would align most closely with T-classification:
T[#]
You completed the skin classification. Blood, lymph node, and visceral classifications are needed for a complete staging of the patient.
Blood (B) Classification
Question 1
Has the patient’s blood been evaluated for the presence of atypical (Sézary) cells?
- The level of peripheral blood involvement has important prognostic significance in Mycosis Fungoides (MF) and Sézary Syndrome (SS)1; ISCL/USCLC/EORTC international guidelines specify that blood evaluation is integral to staging2
- Blood is classified into 3 categories (B0, B1, B2) based on the absolute number of atypical (Sézary) cells in the peripheral blood2
Please choose one:
- ISCL/USCLC/EORTC consensus guidelines recommend flow cytometry as the preferred method for identifying aberrant T cells in the blood and classifying blood tumor burden2
-
Expert tips for ordering flow cytometry
- In the flow cytometry request, specify that CTCL is suspected and/or if there is an existing diagnosis
- Consensus guidelines recommend a minimum of 6 T-cell markers for the flow cytometry panel; it may be helpful to confirm that at least 6-color flow is available3
- Use the same flow center for sequential analyses for consistency4
- Consider consultation with CTCL specialist5
- Be sure to include CBC with differential in the flow cytometry request; absolute lymphocyte counts from CBC will aid with determining B classification2
-
ISCL/USCLC/EORTC consensus guidelines recommend flow cytometry as the preferred method for identifying aberrant T cells in the blood and classifying blood tumor burden2
- Cytopathologic assessment by manual Sézary cell counts may be used; however, it is considered less useful due to the subjective nature of the process1
- Blood evaluation is essential for staging MF and SS; if information on blood classification is missing or unclear, stage cannot be accurately estimated2
- ISCL/USCLC/EORTC consensus guidelines recommend flow cytometry as the preferred method for quantifying abnormal T cells in the blood2
Blood (B) Classification
Question 2
Is the blood classification stated in the pathology or flow cytometry report?
- Blood classification is based on the absolute number of immunophenotypically abnormal T cells in the blood2
-
Consensus guidelines from an international group of flow cytometry experts recommend a minimum of 6 T-cell markers for diagnosing MF/SS, although T-cell panels will vary between institutions3
- CD3, CD4, CD7, CD8, CD26, CD45
-
Loss of CD7 and CD26 are common T-cell abnormalities in MF and SS3
- CD4+/CD7- and/or CD4+/CD26- are common phenotypes seen in MF and SS2
- Keep in mind that flow cytometry protocols and interpretation of results vary between institutions; the expertise of the flow cytometrist is crucial for evaluating blood involvement4
Please choose one:
- Guidelines recommend molecular analysis to detect clonal T-cell receptor (TCR) gene rearrangements to help evaluate blood involvement5
- Sézary syndrome is defined by B2 blood involvement and typical identical TCR gene rearrangements in the blood and skin2
- Clonality testing should be performed by the same method as that for skin2
-
Let’s try a different way to determine the blood classification.
- The absolute value of abnormal lymphocytes should be used to determine B class. If B class is not stated in the report, the absolute value can be determined by calculating the percentage of aberrant lymphocytes identified on flow cytometry multiplied by the total lymphocyte count of the CBC. It may also be calculated by determining the percentage of aberrant CD45 leukocytes/white blood cells (WBC) identified on flow cytometry multiplied by the WBC2
Blood (B) Classification
Question 3
Are absolute counts of abnormal T cells available?
Let’s try a different way to determine the blood classification.
Choose which of the following best describes the quantity of abnormal T cells.
Blood (B) Classification
Question 4
Are percentages of abnormal T cells provided in the pathology or flow cytometry report?
- Either absolute counts or percentage of abnormal lymphocytes are needed to calculate B classification2
- Due to the rarity and complexity of the disease, NCCN guidelines recommend consultation with hematopathologists with expertise in CTCL for assessing blood classification2
Please enter the values in the formula below.
Blood (B) Classification Result
Based on NCCN and ISCL/USCLC/ EORTC consensus guidelines and the information you provided, this patient would align most closely with B-classification:
B[#]
If blood classification is Bx (unable to quantify based on agreed-upon guidelines), TNMB stage cannot be accurately estimated.2
You are almost there—only lymph node and visceral/metastasis classifications are remaining.
- Blood can be further characterized by the designation of A (clone negative or equivocal) or B (clone positive and identical to skin)1
- Molecular analysis to detect clonal TCR gene rearrangements or other assessment of clonality is recommended and can help confirm diagnosis and stage1,2
- Clonal TCR gene rearrangements alone are not sufficient for diagnosis, and results should be interpreted in the context of overall clinical presentation. It is expected that patients with high blood tumor burden (B2) will have identical clones in blood and skin1,2
- Due to the rarity and complexity of the disease, NCCN guidelines recommend consultation with hematopathologists with expertise in CTCL for assessing blood involvement2
Lymph Node (N) Classification
Question 1
Did the clinical examination show evidence of lymphadenopathy or other lymph node abnormalities?
- Lymph nodes must be assessed for accurate staging
- Mycosis fungoides (MF) or Sézary Syndrome (SS) can involve lymph nodes, which may be an indicator of increased risk of progression1,2
- Lymph node assessment is an integral component of the staging criteria1,2
- Palpation of peripheral lymph node regions is an essential component of the complete workup for MF and SS
- Although enlarged lymph nodes may sometimes be indicative of lymph node involvement, other causes should be considered
- Patients with enlarged lymph nodes are at higher risk for disease progression
Lymph Node (N) Classification
Question 2
Does the patient have plaques and patches affecting ≥10% of the BSA (T2b or higher classification)?
- Consider imaging if there is evidence of adenopathy or for skin classification T2b or higher (patches + plaques ≥10% of BSA)1
- Imaging may also be useful if large cell transformation or follicular MF are suspected, for aggressive disease, or for abnormal laboratory studies; also consider imaging for skin classification T2a if clinically indicated1
- Keep in mind that patients with enlarged lymph nodes are at higher risk for progression regardless of T classification2
Lymph Node (N) Classification
Question 3
Have imaging studies of lymph nodes been done?
- NCCN Guidelines suggest C/A/P CT with contrast or integrated whole body FDG-PET CT for patients with palpable adenopathy or abnormal laboratory studies, or for suspected large cell transformation or follicular MF3
- Imaging is recommended for skin classification T3 or T43
- Imaging may be considered for patients with T2b (plaques and patches ≥10% of BSA) with palpable adenopathy or abnormal laboratory studies3
- Imaging may also be considered for skin classification T2a (patches ≥10% of BSA) if there is evidence of progression or accelerated skin disease3
Lymph Node (N) Classification
Question 4
Are the imaging results suggestive of lymph node involvement?
- Clinically abnormal nodes are defined as >1.5 cm in longest diameter1
Lymph Node (N) Classification
Question 5
Has the patient been referred for a lymph node biopsy?
- ISCL/USCLC/EORTC international consensus guidelines recommend lymph node biopsy for clinically abnormal nodes (defined as >1.5 cm in longest diameter)1
- Evaluation of nodal biopsies by a pathologist with expertise in CTCL is recommended1
- Biopsy is required to help confirm lymph node involvement1
- According to consensus guidelines, Nx may be used for abnormal lymph nodes without histologic confirmation1
Lymph Node (N) Classification
Question 6
Did the pathology report indicate lymph node involvement?
Please select an N classification if included in the pathology report.
If N class was not stated, select Nx
Lymph Node (N) Classification Result
Based on NCCN and ISCL/USCLC/EORTC consensus guidelines and the information you provided, this patient would align most closely with N-classification:
N[#]
If N classification is Nx (clinically abnormal but no pathologic determination of lymph nodes), TNMB stage cannot be accurately estimated.1 Consultation with a CTCL expert is recommended for diagnosing and staging MF and SS.2
You are almost there—only visceral/metastasis classification is remaining.
-
Consensus guidelines define lymph node classifications as follows1:
- Nx = clinically abnormal but no pathologic determination of lymph nodes
- N0 = no evidence of lymph node involvement
- N1 = Dutch grade 1 (dermatopathy lymphadenopathy) or NCI lymph node classification 0-2
- N2 = Dutch grade 3 or NCI lymph node classification 3
- N3 = Dutch grade 3-4 or NCI lymph node classification 4
- Stage can be further characterized by a designation of A (clone negative or equivocal) or B (clone positive and identical to skin)
- Results should be interpreted in the context of overall clinical presentation
-
NCI-VA lymph node classification
- LN0 = no atypical lymphocytes
- LN1 = occasional and isolated atypical lymphocytes (not arranged in clusters)
- LN2 = many atypical lymphocytes or in 3-6 cell clusters
- LN3 = aggregates of atypical lymphocytes; nodal architecture preserved
- LN4 = partial/complete effacement of nodal architecture by atypical lymphocytes or frankly neoplastic cells
-
Dutch criteria for lymph nodes
- Grade 1 = dermatopathic lymphadenopathy
- Grade 2 = early involvement by MF (presence of cerebriform nuclei >7.5 µm)
- Grade 3 = partial effacement of lymph node architecture; many atypical cerebriform mononuclear cells
- Grade 4 = complete effacement of lymph node architecture
Metastasis (M) Classification
Question 1
Does patient have advanced disease (eg, skin classification T3 or higher [tumors, erythroderma], high blood burden [B2])?
- Visceral involvement is rare but may be present in advanced disease1
-
BONE MARROW BIOPSY IS NOT STANDARD FOR CTCL STAGING
- NCCN and ISCL/USCLC/EORTC guidelines specify that bone marrow biopsy should only be done under certain circumstances
Metastasis (M) Classification
Question 2
Did the clinical examination show signs of visceral involvement (eg, liver, spleen enlargement, evidence of masses, or other evidence of systemic disease)?
- ISCL/USCLC/EORTC consensus guidelines include evaluation for visceral involvement as part of the TNMB staging criteria1
Metastasis (M) Classification
Question 3
Has imaging been done to assess for visceral involvement?
- Imaging is recommended for T3 or higher1,3
- Imaging may be considered for ≥T2 disease if there is clinical suspicion of visceral involvement1,3
- NCCN and ISCL/USCLC/EORTC consensus guidelines recommend C/A/P CT with contrast or integrated whole-body FDG-PET CT to assess for visceral involvement1,3
- Imaging is recommended for suspected visceral disease with organ involvement (eg, spleen, liver) for accurate staging1,3
Metastasis (M) Classification
Question 4
Are imaging results suggestive of visceral involvement?
Metastasis (M) Classification
Question 5
Has the patient been referred for biopsy?
Visceral/Metastasis (M) Classification Result
Based on the information you provided, this patient would align most closely with M-classification:
M[#]
If M classification is Mx (visceral involvement neither confirmed nor refuted by available pathologic or imaging assessment), TNMB stage cannot be accurately estimated.1 Consultation with a CTCL expert is recommended for diagnosing and staging MF and SS.2
Thank you for taking the time to complete all 4 classifications.
Based on the information provided, this patient likely has
Tx Nx Mx BxWhich corresponds to TNMB stage:
XXTNMB stage cannot be accurately estimated
| TNMB classification for Mycosis Fungoides/ Sézary Syndrome6 |
|||||
|---|---|---|---|---|---|
| Clinical stage | Classification | ||||
| T | N | M | B | ||
IA |
1 |
0 |
0 |
0,1 |
|
IB |
2 |
0 |
0 |
0,1 |
|
IIA |
1,2 |
1,2 |
0 |
0,1 |
|
| Advanced Disease | IIB |
3 |
0-2 |
0 |
0-1 |
IIIA |
4 |
0-2 |
0 |
0 |
|
IIIB |
4 |
0-2 |
0 |
1 |
|
IVA1 |
1-4 |
0-2 |
0 |
2 |
|
IVA2 |
1-4 |
3 |
0 |
0-2 |
|
IVB |
1-4 |
0-3 |
1 |
0-2 |
|
Evaluation Summary
Complete the short form below to receive
a summary of this evaluation.
All fields are required.
If any of the compartmental classifications were not established (ie, Nx, Bx, Mx), then TNMB staging cannot be calculated.1
Due to the complexities involved in diagnosing and staging MF and SS, it is strongly advised in the consensus guidelines to consult a pathologist with expertise in CTCL or to refer to a CTCL center for suspected cases. A multidisciplinary team approach is essential for optimal patient management.2
COMM-US-ONC-0101
Due to the complexities involved in diagnosing and staging Mycosis Fungoides and Sézary Syndrome, it is strongly advised in the NCCN consensus guidelines to consult a specialist with expertise in CTCL or to refer to a CTCL center for suspected cases.2
CTCL, cutaneous T-cell lymphoma; EORTC, European Organisation for Research and Treatment of Cancer; ISCL, International Society for Cutaneous Lymphomas; NCCN, National Comprehensive Cancer Network; TNMB, tumor, node, metastasis, blood; USCLC, United States Cutaneous Lymphoma Consortium.
References: 1. Olsen EA, Whittaker S, Willemeze R, et al. Primary cutaneous lymphoma: recommendations for clinical trial design and staging update from ISCL, USCLC, and EORTC. Blood. 2022;140(5):419-437. 2. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Cutaneous Lymphomas V.2.2026. © National Comprehensive Cancer Network, Inc. 2026. All rights reserved. Accessed March 3, 2026. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.